
I’m going to jump out of my strength coach lane and attempt to play physical therapist for a minute, I am neither qualified (DPT) nor endorsed to discuss this topic, I am just playing word vomit with my thoughts.
Asking yourself “Does it hurt” will help you determine whether or not training is safe for you if you have an injury. The important thing to remember is that there are only two possible responses to the question “does it hurt?” No matter how much you might like the activity, if you respond “yes,” you are not ready for it. There is an underlying issue that needs to be understood and addressed before there is a return to that activity.
It shouldn’t hurt to exercise. This seems straightforward, yet athletes (and the average person) frequently ignore pain before attempting to explain it away. Just to be clear, we are not referring to the discomfort of getting hit by a pitch, having a shot blocked, or getting destroyed by a one rep max. This conversation focuses on the discomfort felt during exercise. This is the knee discomfort felt during a squat or the shoulder pain felt during a bench press.
It’s also critical to remember that discomfort is frequently experienced at the conclusion of a set of a strength exercise or a challenging cardio session. In the two days after an intense workout, delayed onset muscle soreness frequently causes further agony. That is typical. Ideally, this discomfort would only last maybe two days and only affect muscles with increased damage and inflammation to that muscle. That pain should not radiate and be felt chronically in the tendons and joint of limbs.
Pain at the onset of exercise, however, is neither normal nor healthy and is usually indicative of a problem. Just because the pain decreases or goes away as you warm up does not change my thought process. Progression in any strength exercise should be based on being able to go through a full, pain-free range of motion. An exercise can potentially produce muscle soreness, but joint soreness, tendon soreness, or insertion point pain is the sign of a problem. If you need to change or reduce your range of motion, this is also a sign of a problem.
Rehab protocol should be handled in three phases: “Release – Open – Anchor”
Here are my thoughts on rehab protocol specifically for the shoulder. I have an interest in softball and baseball mechanics in relation to injury and possible tendinopathy mechanisms.
Before we get into the training applications, allow me to first give a brief outline for why fascial concepts should be considered in a sport performance and rehab setting. Fascia is the connective tissue that plays important roles in biological structure, movement, and function. In a laymen’s sense, you can think of fascia as being a global connective tissue that, quite literally, connects us from head to toe. Fascia is also highly enriched with proprioceptive bodies and free nerve endings that play critical roles in detecting external stimuli, movement coordination, and even spatial orientation.
Heres the layout for Fascia in our bodies
- The skin covers our body and under the epidermis lies the first loose fascia superficial layer that houses the subcutaneous fat tissue – the outermost shell, so to speak. It ensures firmness of the skin and mobility to the underlying structures. Whether one can actually speak of a uniform fascial class is scientifically controversial.
- Below lies the deep fascia layer (fascia profunda) as a firmer second shell. It gives shape to the body – a cover, like a diving suit.
- Below are the muscles, individual muscle bundles, even the muscle fibers packed in fascia. The muscular connective tissue (myofascia) prolongs and thickens in tendons, form flat structures, come to light here and there thicker, firmer, are interwoven with each other and with ligaments and capsules, but equally separated from each other.
How does this play in to the role of rehab protocol of the shoulder. Self-myofascial release or SMR involves applying the right amount of pressure to muscles and the fascia to help relieve pain, discomfort, and free up fascial tension localized in that area. When done properly, SMR techniques do not only provide shoulder pain relief, but also restores shoulder mobility and joint range of motion, all of which should be considered before any movement is applied and tension is increased due to muscular inflammation and tensile stress.
SMR techniques involve applying pressure to muscles and fascia to help break up lines of tissue that can be inflamed. These techniques can resolve shoulder mobility and impaired movements when done correctly. However, the technique must be done correctly to avoid exacerbating an already bad condition. The benefits of SMR can be felt almost immediately if done right.
The more common SMR techniques involve using a foam roller, and some of these techniques include
- Latissimus rolls
- Pec rolls
- Trapezius rolls
Before any exercises are completed SMR is recommended to aid in increased mobility, inflammation and stiffness of the shoulders. This is the “Release” stage

“Movement is medicine,” right? As much as coaches and practitioners like to attribute soreness and tightness to just being a part of the process, it cannot be lost on us that expediting the return to optimal is very much a part of our fundamental duty. There’s no doubt that athletes will get beat up during the season and throughout particular phases of the training cycle. However, considering the optics and fundamental roles of a strength coach, it can be easy to slip into autopilot with restorative modalities such as a haven of mobility exercises and “recovery” training sessions.
The “open” in protocol refers the opening of the shoulder girdle, thoracic spine, and rib expansion. Another situation is with athletes who’ve had major surgeries or injuries. The additional fibrous tissue (collagen) surrounding the injured site can be needed for stability and structure. “Protective tension,” if we aggressively seek to “undo” this tension, it can destabilize the athlete while potentially affecting confidence in the area negatively. The main point being, don’t get carried away with overstretching and mobilizing every athlete you see on equal terms—not all athletes need to stretch/mobilize the same.
Factors that influence tightness or stiffness of joints:
- Neurological function
- CNS/PNS stability
- Tendon Stiffness
- Endocrine levels of inflammation
- Metabolic levels
- External stress
Stiffness or tightness of muscles and joints needs to be address in a hierarchal order. The first place to start is always with the central governor: the brain and central nervous system (CNS). As Stu McGill has said, “Stretching is just playing with the neurology.” What he means by this, as an example, is if an athlete is in true sympathetic overdrive (i.e., overtraining) resulting in a constant state of tightness, we can do all the stretching and mobility work in the world, but until the sympathetic (SNS) and parasympathetic (PSNS) nervous system balance is addressed, the athlete will still feel sore/tight, leaving our efforts in vain.
Working down the hierarchy, we have a few additional considerations as well. The distribution of collagen fibers (fascial densification), muscle fiber type ratio, tendon length and insertion, and localized circulation are a handful of additional factors that may have a significant influence on the sensation of stretching and how we approach treating it. As with anything else, these systems, ratios, and functions are different across different populations/individuals; likewise, the approach must be modified to fit the specific demands.
Movement in the “open” period involves exercises and modalities that will accomplish what we discussed: lower neurological state of exhaustion, stress and lengthening of tendons and muscle belly, decrease tendon stiffness, and will lower endocrine and metabolic levels. These movements look like
- Blackburn Series
- Banded Shoulder Series
- T-Spine Rotational Exercises
- Extension and Flexion of the Spine
- Oscillatory Work
- AFSM Work
- Tempering
The key with “opening” joints, is limiting additional stress before the real stress of exercise
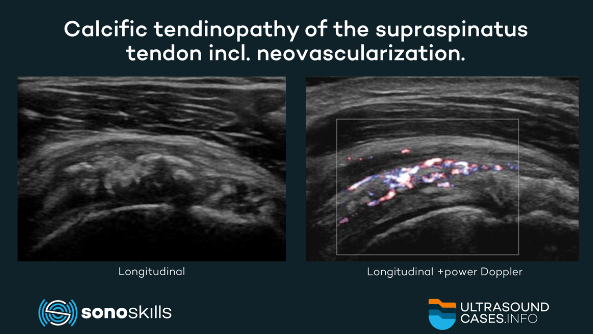
Tendons are generally poorly vascularized, while certain regions—those most prone to injury—are almost avascular (lacks blood vessel). This can be considered an evolutionary ‘design failure’ that makes tendons susceptible to chronic and acute injuries. As a consequence, healthy tendons have a virtually non-existent tissue turnover throughout adulthood. However, somewhat paradoxically, tissue turnover is increased in tendinopathic tendons.
Tendinopathy is a general term that describes tendon degeneration characterized by a combination of pain, swelling, and impaired performance. Common sites include the rotator cuff (supraspinatus tendon), wrist extensors (lateral epicondyle) and pronators (medial epicondyle), patellar and quadriceps tendons, and Achilles tendon.
“Anchoring” of rehab protocol includes exercises that increase satellite cell projection to the muscle and tendon of that area. This is caused by tension stress to the area caused by exercise induced stimulus or reflex stretch. Exercises in this area will have a ceiling of 200 reps or extreme isometric stress. We want to induce the most damage we can without illiciting greater tendinopathy. This will impair performance if we do not handle volume load correctly. Isometric hypertrophy to the generalized areas will involve exercises like
- Non-Dominant drop catches
- Dips/Dip Shrugs
- External Rotation in the saggital plane
- Extreme Isometrics in disadvantageous positions
- Retraction of the shoulder blades
- Flys in advantageous positions
- Maxwell shoulder ISOs
- Flexion and Extension in short range
The “anchor” series of rehab needs to include exercise that is going to cause tissue and muscle damage without enhancing tendinopathy and increasing further damage. In consideration of the athlete, there might not be any other time to stress the neuromuscular system in a better time than after an injury, and non-dominant side awareness might also help get some varied training into their routine.
One plausible explanation for some of these potential benefits from non-dominant triphasic training might be the increases in EMG activity during concentric contractions compared to eccentric. Once again, as we correlate this to our athlete, if the goal of speed training is to really charge the neuromuscular system, incorporating Isometric contractions would stand to increase the activity of the muscles utilized in the task. It also will enhance tissue quality in the long term.
General physical preparedness in protocol should serve as a base of fundamental movements executed to facilitate fundamental adaptations. A lengthy period away from the weight room, for any reason, should be met with due care and attention when it comes to returning our athletes to a properly structured, well-designed strength and conditioning program.
Here is a sample 4 week rehab protocol to use with shoulder rehab:
References
KM;, A. G. R. C. D. C. H. F. B. (n.d.). Skeletal muscle hypertrophy in response to isometric, lengthening, and shortening training bouts of equivalent duration. Journal of applied physiology (Bethesda, Md. : 1985). Retrieved February 9, 2023, from
Rintoar. (2020, October 22). How to relieve shoulder pain using myofascial release techniques: Dynamic Physiotherapy & Sports Injury Clinic. Dynamic Physiotherapy & Sports Injury Clinic Inc. Retrieved February 9, 2023, from
Järvinen, T. A. H. (2020, January 1). Neovascularisation in tendinopathy: From eradication to stabilisation? British Journal of Sports Medicine. Retrieved February 9, 2023, from
Academy, F. T. (2020, December 17). What is fascia? FASCIA TRAINING ACADEMY. Retrieved February 9, 2023, from
Shoulder tendinopathy. Shoulder Tendinopathy | UVA Health. (n.d.). Retrieved February 9, 2023, from
James, J. (2020, April 28). How to return to Strength Training (a guide for athletes and practitioners). SimpliFaster. Retrieved February 9, 2023, from
Sports News
website focused on news and information about the world of football. This is one of the popular websites in Indonesia accessed by sports fans, especially football enthusiasts, to get quick and reliable information.


